As prescription drug expenditures continue to exert pressure on state and federal budgets, the Trump administration has launched an ambitious initiative aimed at fundamentally altering how Medicaid procures pharmaceuticals. The "GENEROUS" (GENErating cost Reductions fOr U.S. Medicaid) model represents a bold attempt to import international price benchmarks into the American healthcare landscape. By tying Medicaid rebates to the prices paid in eight comparable nations, the administration seeks to eliminate the significant price disparity that has long seen U.S. patients and taxpayers paying substantially more than their international counterparts.
While the program holds the promise of billions in potential savings, its actual impact remains a subject of intense debate. The complexity of existing rebate structures, the voluntary nature of manufacturer participation, and the opaque details of confidential agreements create a high degree of uncertainty regarding whether this model will deliver on its multi-billion-dollar projections.
Main Facts: The Architecture of the GENEROUS Model
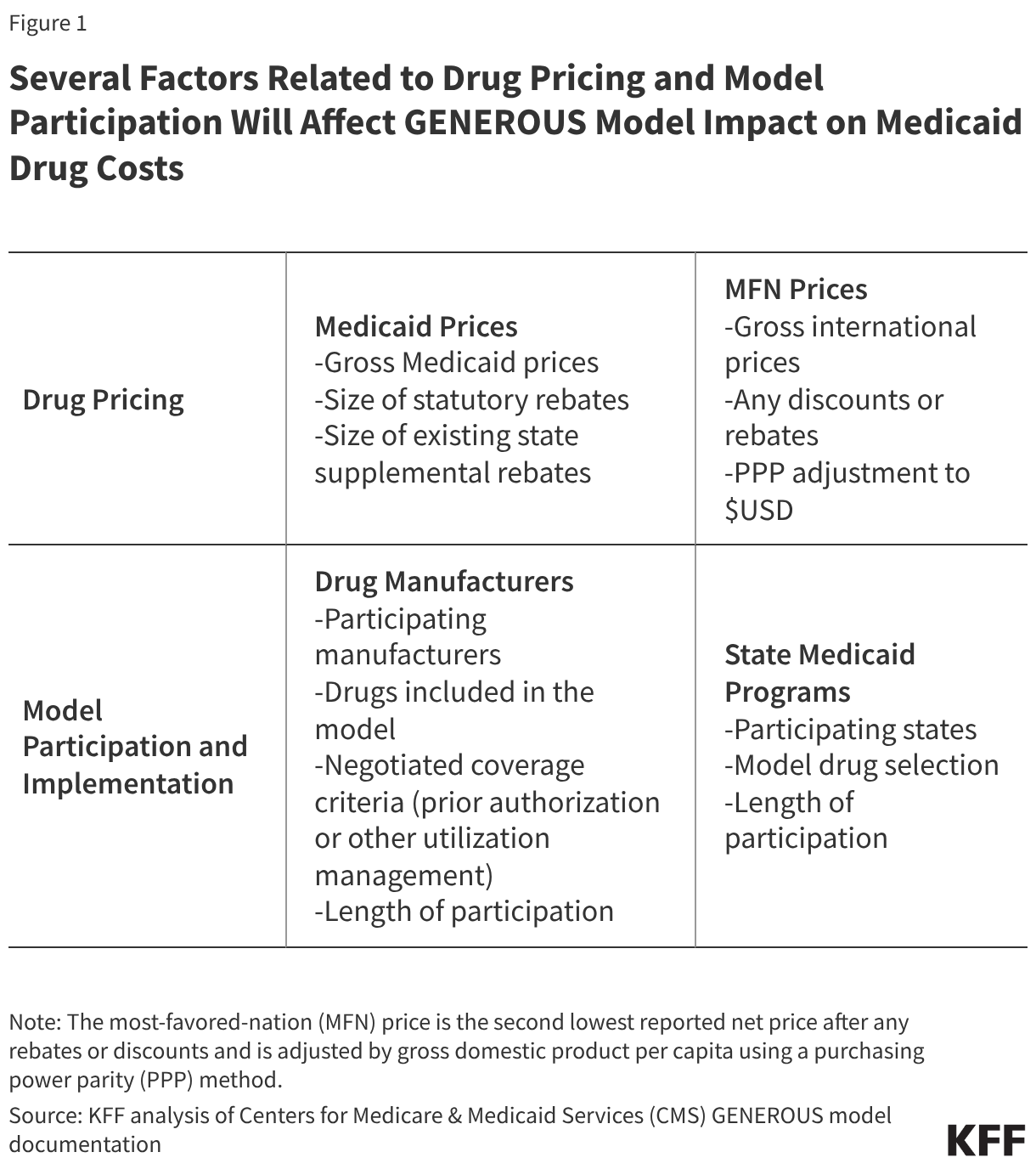
At its core, the GENEROUS model is a payment innovation designed to leverage international pricing to lower the net cost of brand-name drugs for Medicaid. Launched by the Centers for Medicare & Medicaid Services (CMS) in January 2026, the model targets single-source and innovator multiple-source drugs.
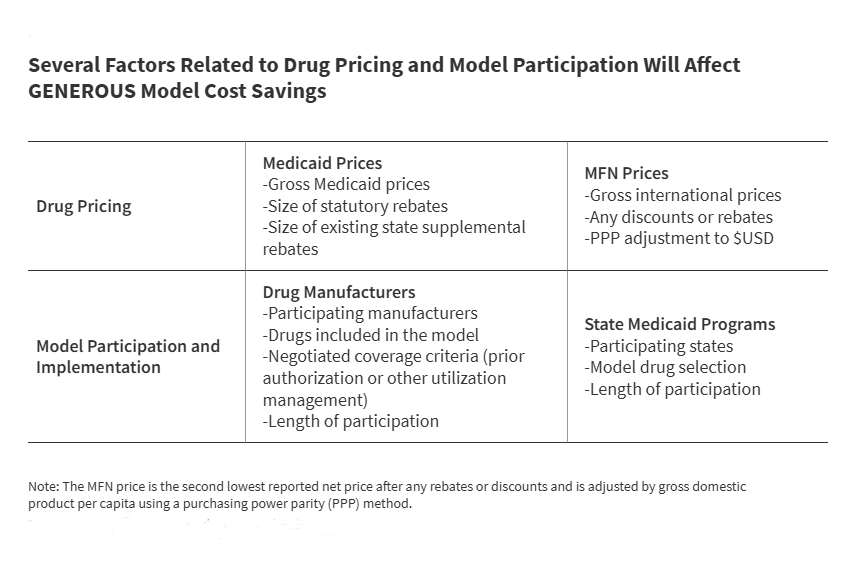
The mechanism is straightforward in theory: CMS calculates a "Most-Favored-Nation" (MFN) price for a given drug based on pricing data from eight nations: the United Kingdom, France, Germany, Italy, Canada, Japan, Denmark, and Switzerland. This MFN price—the second-lowest net price among these countries, adjusted for local purchasing power—becomes the benchmark. Manufacturers who participate in the model agree to provide supplemental rebates that effectively bring the Medicaid net price down to this MFN level.
The model is voluntary for both pharmaceutical manufacturers and individual states. For manufacturers, the incentive is tied to broader trade and regulatory negotiations, including a three-year reprieve from specific pharmaceutical tariffs. For states, the incentive is the potential for deeper discounts on high-cost therapies that currently strain state Medicaid budgets.
Chronology: A Timeline of Implementation and Expansion
The path to the GENEROUS model has been marked by rapid development and multiple adjustments to timelines, reflecting the complexities of coordinating between federal regulators, state agencies, and the pharmaceutical industry.
- September – December 2025: The administration secures a series of high-profile "Most-Favored-Nation" pricing agreements with major pharmaceutical entities, including Pfizer and AstraZeneca, establishing the foundational momentum for the model.
- January 2026: CMS officially launches the GENEROUS model, setting an initial application deadline for manufacturers of March 31, 2026.
- Spring 2026: Recognizing the administrative hurdles involved, CMS extends the manufacturer application deadline twice—first to April 30 and subsequently to June 11, 2026.
- April 2026: The White House releases a pivotal report estimating that a voluntary MFN framework could save the Medicaid program approximately $64.3 billion over the next decade.
- July – August 2026: The focus shifts to states, which must submit applications by July 31 and finalize participation agreements by August 31, 2026.
- 2026–2030: The model is scheduled to operate for a five-year demonstration period, subject to ongoing evaluation and potential renegotiation of terms.
Supporting Data: The Disparity in Drug Pricing
The economic justification for the GENEROUS model rests on a well-documented observation: prescription drugs in the United States often cost three times as much as they do in other developed nations.
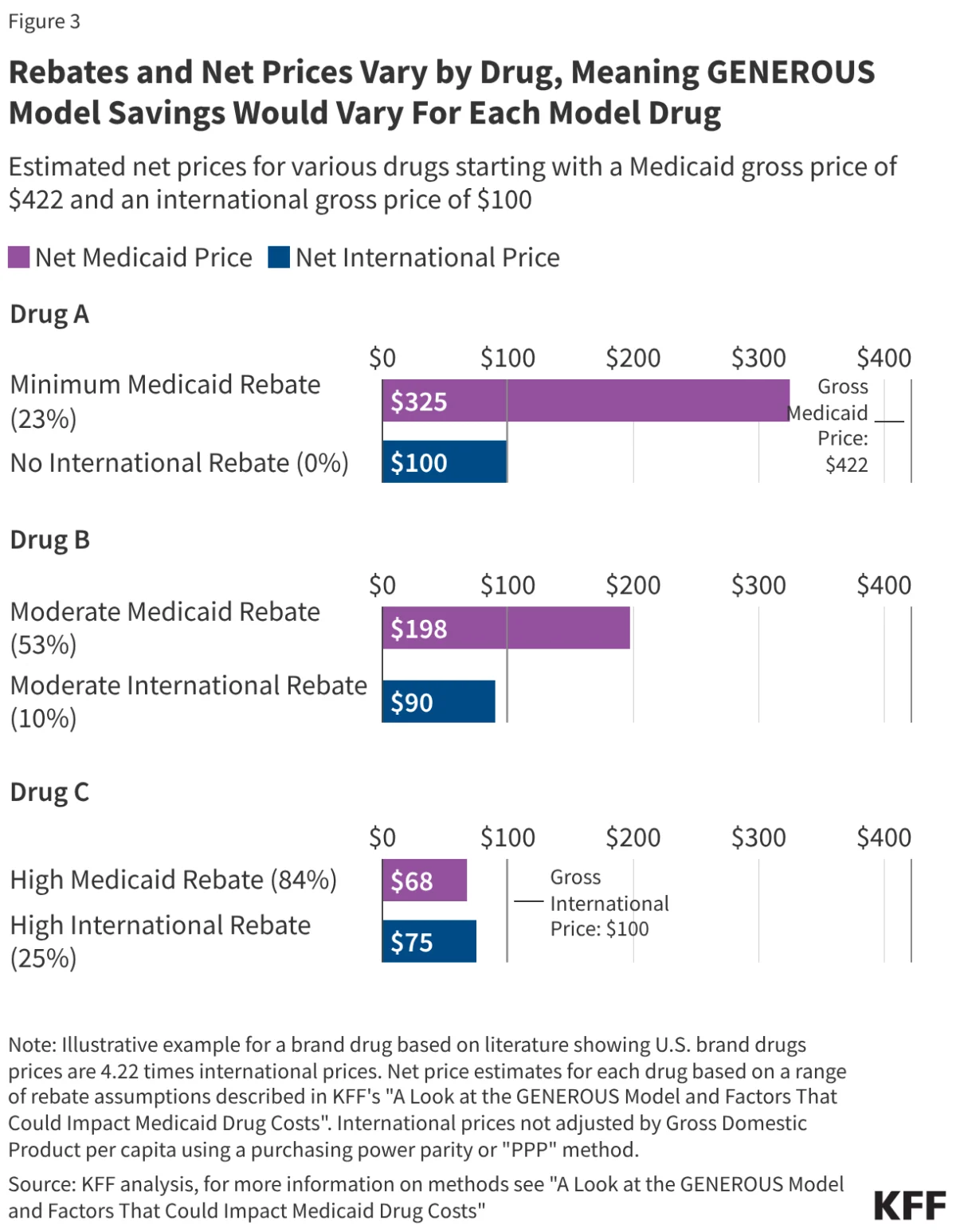
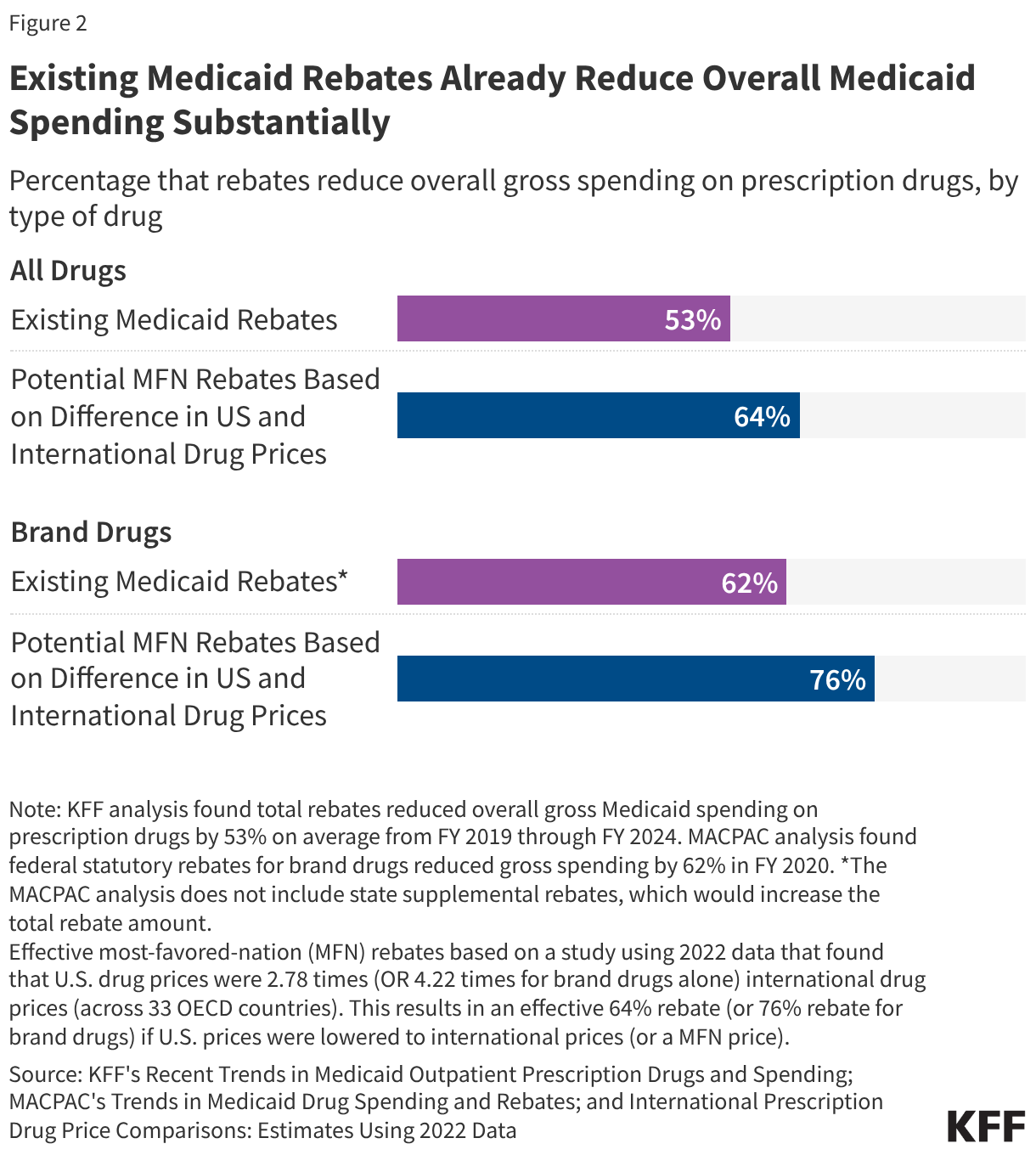
According to various studies, while Medicaid already benefits from a robust rebate system—reducing gross spending by an average of 53% between 2019 and 2024—there remains a significant "price gap." For brand-name drugs, this gap can be even more pronounced. Research indicates that if the U.S. were to successfully align its prices with international benchmarks, the resulting discount could equate to a 64% to 76% reduction off current gross U.S. prices.
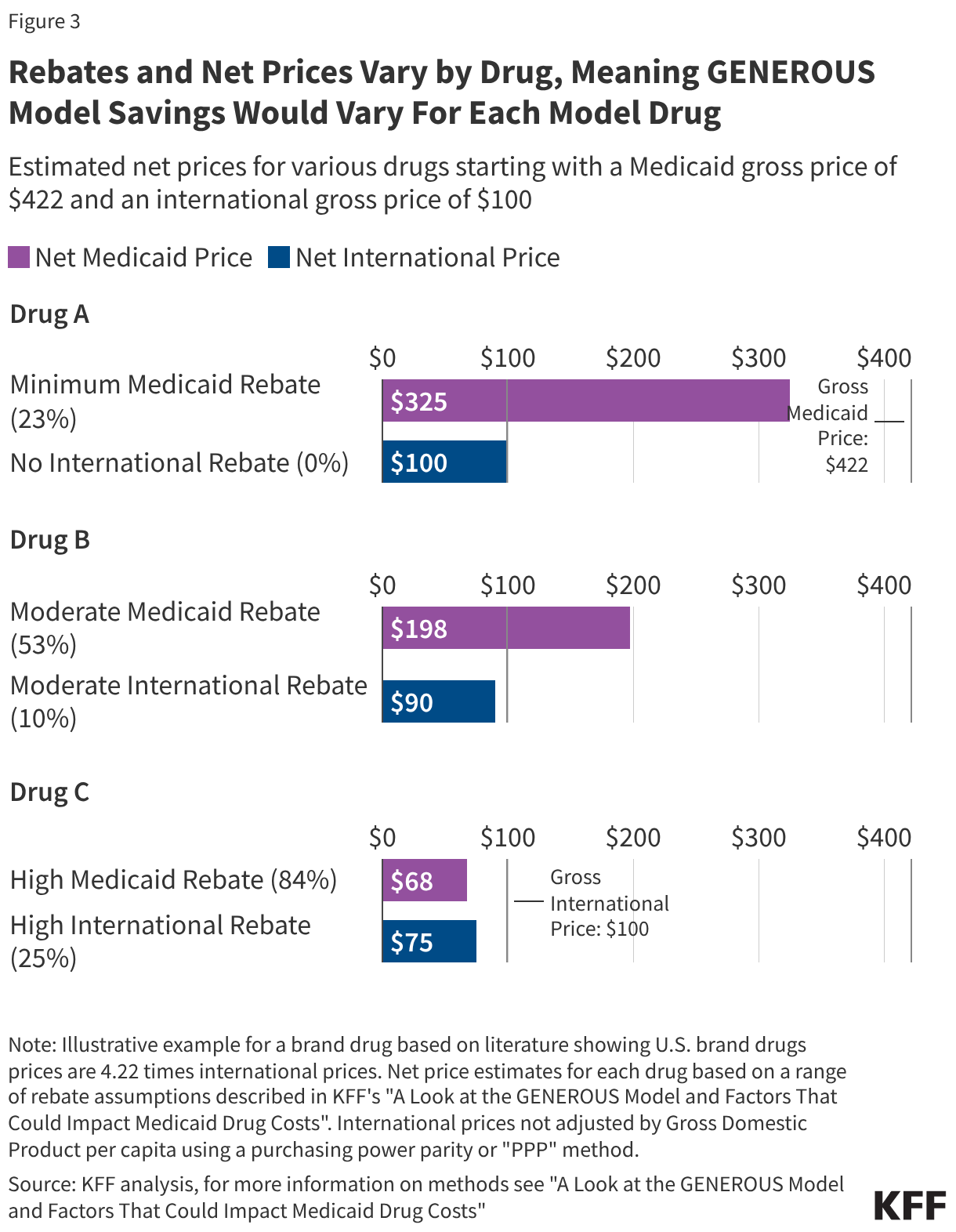
However, the data also highlights the "diminishing returns" factor. Because Medicaid already negotiates significant statutory and supplemental rebates, some drugs are already priced at or near cost-recovery levels. For example, drugs like the anticoagulant Eliquis already benefit from near-100% total rebates in some instances. Consequently, the GENEROUS model will likely see the highest savings on newer, highly specialized therapies where competition is scarce and current Medicaid rebates are relatively low.
Furthermore, the concentration of spending is a critical data point: the top 50 drugs account for over one-third of all Medicaid drug spending. The success of the model will hinge on whether CMS can secure participation for these high-utilization, high-cost medications.
Official Responses and Stakeholder Perspectives
The reception of the GENEROUS model has been mixed, reflecting the competing interests of federal policymakers, state administrators, and the pharmaceutical industry.
The Federal Position: The White House and CMS contend that the model is a necessary tool to restore fairness to the U.S. drug market. By leveraging the threat of tariffs and the promise of a predictable, long-term regulatory environment, the administration argues that it is forcing manufacturers to end "price gouging" of the American taxpayer.
State Agency Perspectives: Many state Medicaid directors are cautious. While they are eager for any mechanism that alleviates the pressure of rising pharmacy costs, they are wary of the administrative burden. The requirement to adopt "uniform coverage criteria"—which may include standardized prior authorization or step therapy protocols—could clash with state-specific clinical policies that have been refined over years. States must weigh the potential for supplemental rebates against the possibility that standardized criteria might be more restrictive or less clinically appropriate for their specific patient populations.
Industry Concerns: Pharmaceutical companies have raised concerns regarding the transparency of the MFN pricing data and the long-term impact on R&D. While some have signed onto the agreements to avoid the immediate impact of tariffs, there is underlying tension regarding the "confidential" nature of these deals. Critics argue that without full transparency, it is impossible to verify if these deals provide genuine value or simply create a "black box" of pricing that serves political optics rather than long-term fiscal health.
Implications: A New Era for Medicaid Pharmacy Management?
The implementation of the GENEROUS model carries significant implications for the future of healthcare policy in the United States.
1. The Shifting Landscape of Medicaid Savings
The primary implication is a fundamental change in the "math" of Medicaid pharmacy spending. If successful, the model will shift the focus from traditional, state-by-state supplemental rebate negotiations toward a centralized, international benchmark. This could lead to a more uniform pricing environment, but it risks creating a two-tiered system where only participating states realize these benefits.
2. Impact on Clinical Access
The standardization of coverage criteria is perhaps the most overlooked aspect of the model. By negotiating uniform prior authorization and step therapy, CMS is effectively creating a national standard for access to certain drugs. While this could reduce administrative overhead, it may also limit the ability of individual states to tailor drug access based on the specific health needs and demographics of their Medicaid enrollees.
3. Long-Term Market Effects
There is a legitimate concern regarding how the model will influence global markets. If the U.S. shifts to an MFN pricing structure, other nations may find their own leverage diminished, potentially leading to price increases globally. Furthermore, as the tariff-based "carrots and sticks" approach expires after the three-year mark, it remains unclear whether manufacturers will maintain their participation without the threat of trade penalties.
4. Transparency and Accountability
The lack of public detail regarding the specific terms of the MFN agreements continues to be a point of friction. With the Senate Finance Committee and other legislative bodies pressing for more data, the administration faces increasing pressure to demonstrate that the model is not merely a short-term fiscal fix but a sustainable approach to drug pricing.
Conclusion
The GENEROUS model is a significant, albeit experimental, step toward addressing the rising costs of prescription drugs within the Medicaid program. By attempting to bridge the gap between U.S. pricing and international standards, the Trump administration has signaled a willingness to use aggressive trade and regulatory tools to achieve budgetary goals.
However, the ultimate success of the program remains contingent on several variables: the willingness of pharmaceutical giants to maintain participation, the ability of states to navigate the complex trade-offs between standardized criteria and localized needs, and the long-term sustainability of the pricing benchmarks. As the August 2026 deadline for state participation approaches, stakeholders across the healthcare spectrum will be watching closely to see if the GENEROUS model can truly "generate cost reductions" or if it will face the same hurdles that have historically complicated attempts to import foreign drug pricing models to the United States.
The path forward requires a delicate balance: achieving the fiscal responsibility required by taxpayers while ensuring that the most vulnerable populations continue to have access to the lifesaving medications they depend on. Whether the GENEROUS model provides this balance or creates new inefficiencies is a question that will only be answered as the five-year demonstration period unfolds.