On July 1, 2026, the landscape of Medicare coverage will shift significantly as the Centers for Medicare & Medicaid Services (CMS) prepares to launch a landmark, albeit temporary, initiative: the Medicare GLP-1 Bridge. This program represents a major policy pivot, creating a pathway for millions of beneficiaries to access high-demand weight-loss medications—drugs that have historically been excluded from standard Medicare Part D coverage due to long-standing statutory prohibitions.
While the program is slated to operate for only 18 months—concluding in December 2027—the introduction of the Bridge marks a critical moment in the ongoing debate over the role of federal health insurance in addressing the national obesity epidemic.
The Core Facts: What is the Medicare GLP-1 Bridge?
The Medicare GLP-1 Bridge is a temporary, demonstration-based program designed to provide coverage for specific GLP-1 receptor agonists used for weight management. These drugs include Wegovy, Zepbound, and Foundayo.
Crucially, the program does not alter the underlying law that prohibits Medicare from covering weight-loss drugs. Instead, the Biden-Harris administration is utilizing its Section 402 demonstration authority—a regulatory tool that allows CMS to test innovative payment and service delivery models that have the potential to improve quality of care or reduce spending. By operating outside of the traditional Part D payment system, CMS can bypass statutory roadblocks to deliver medication directly to those who need it most.
Key Program Features:
- Duration: July 2026 through December 2027.
- Copayment: Eligible beneficiaries will pay a flat $50 monthly copayment.
- Financial Structure: Importantly, these costs will not contribute to a beneficiary’s Part D deductible or their annual out-of-pocket spending cap. Additionally, the Low-Income Subsidy (LIS) assistance does not apply to this specific bridge program.
- Administrative Hurdle: Prescribing clinicians must undergo a rigorous prior authorization process, attesting that the medication is for weight management and confirming that the patient does not have underlying conditions that would otherwise qualify them for GLP-1 coverage under standard Part D.
Clinical Criteria: Who Qualifies?
The eligibility criteria for the Bridge program are notably specific, balancing the need for broad access with the necessity of fiscal responsibility. While the FDA has approved these medications for adults with a BMI of 30 or higher (or 27 or higher with comorbidities), the Bridge program adds a layer of clinical prioritization.
To qualify, a beneficiary must meet one of the following clinical profiles:
- High BMI: A BMI of 35 or more.
- BMI + Comorbidities: A BMI of 30 or more accompanied by heart failure with preserved ejection fraction, uncontrolled hypertension, or chronic kidney disease (stage 3a or above).
- Overweight + Specific Risks: A BMI of 27 or more with pre-diabetes, a history of myocardial infarction, stroke, or symptomatic peripheral artery disease.
The Exclusion Criteria
The program is strictly designed for those who cannot currently access these drugs through existing Medicare channels. Consequently, individuals who already have a diagnosis for conditions that qualify for GLP-1s under Part D—specifically type 2 diabetes, obstructive sleep apnea (OSA), or noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH)—are excluded. This is a deliberate "firewall" to prevent the migration of patients from standard Part D coverage into the temporary Bridge program, which would effectively increase federal spending without expanding access.
Chronology and Development
The road to the July 2026 launch has been marked by mounting pressure from patient advocacy groups, pharmaceutical manufacturers, and clinical organizations arguing that the obesity epidemic is a primary driver of chronic disease in the Medicare population.
- Early 2024: Intense lobbying efforts began to highlight the disconnect between clinical guidelines—which recommend GLP-1s for obesity—and Medicare’s restrictive coverage policies.
- Late 2025: CMS began evaluating the feasibility of using Section 402 demonstration authority to address the gap.
- Early 2026: Following the formal announcement of the Bridge program, CMS began developing the administrative infrastructure, including the prior authorization protocols and data tracking mechanisms.
- July 1, 2026 (Launch): The program officially opens, allowing clinicians to begin the authorization process for eligible patients.
- December 31, 2027: The program sunset date. At this point, the government is expected to evaluate the clinical outcomes and financial impact of the program to determine if a permanent, broader policy change is warranted.
Supporting Data: The Scale of the Population
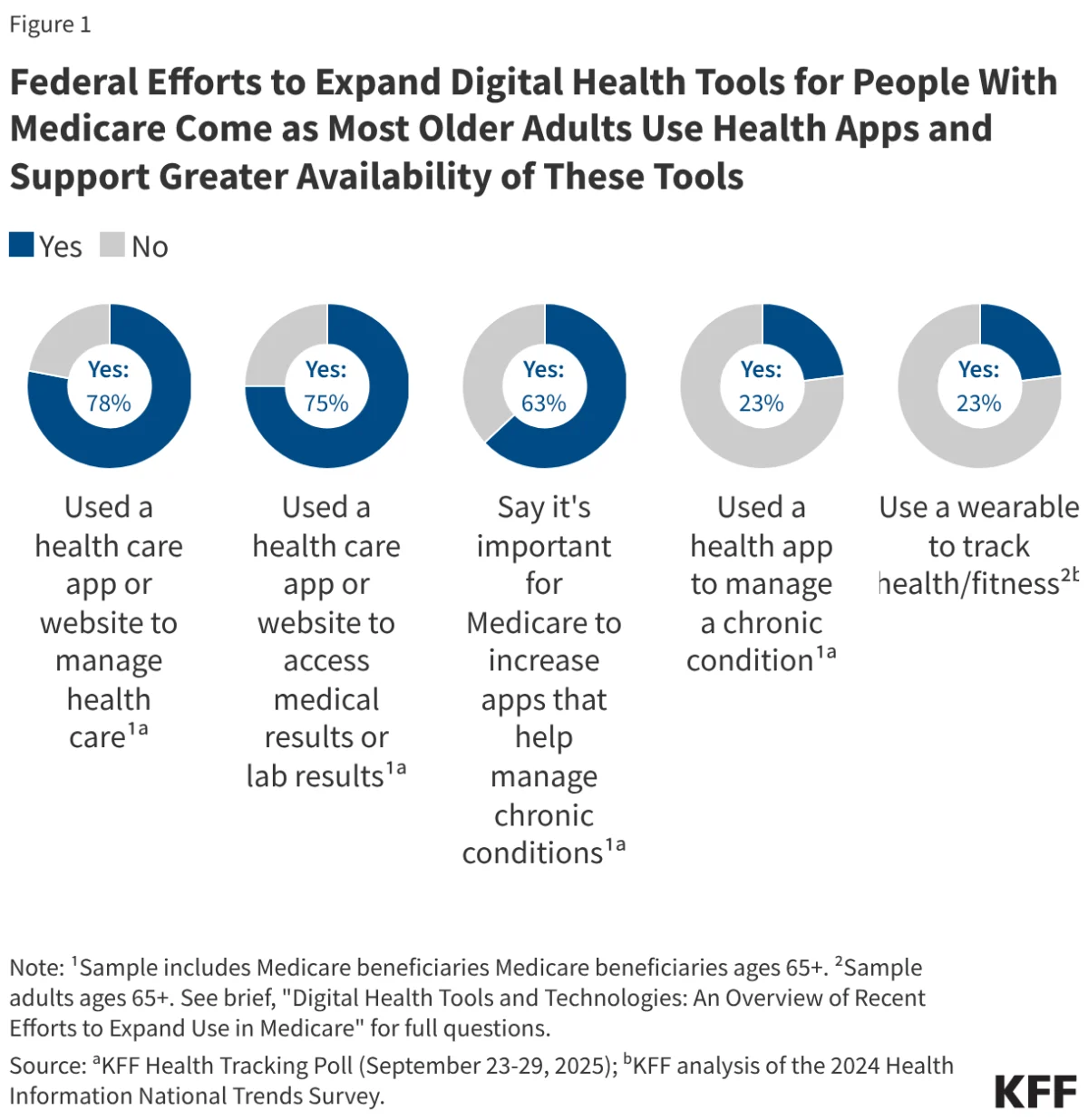
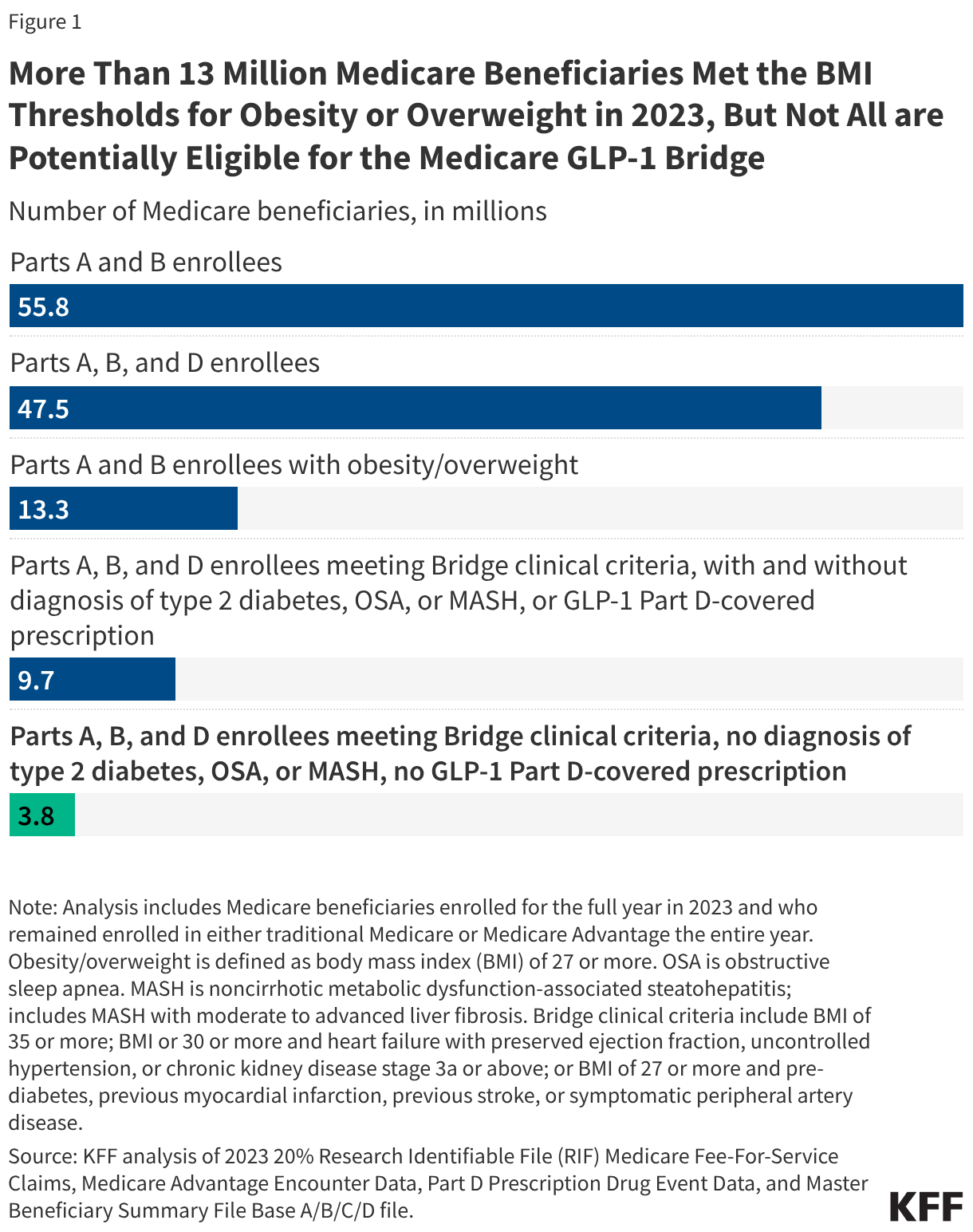
Data provided by recent KFF analyses offers a window into the potential reach of the Bridge program. In 2023, approximately 13.3 million Medicare beneficiaries—about 24% of the total population—met the basic BMI thresholds for obesity or overweight.
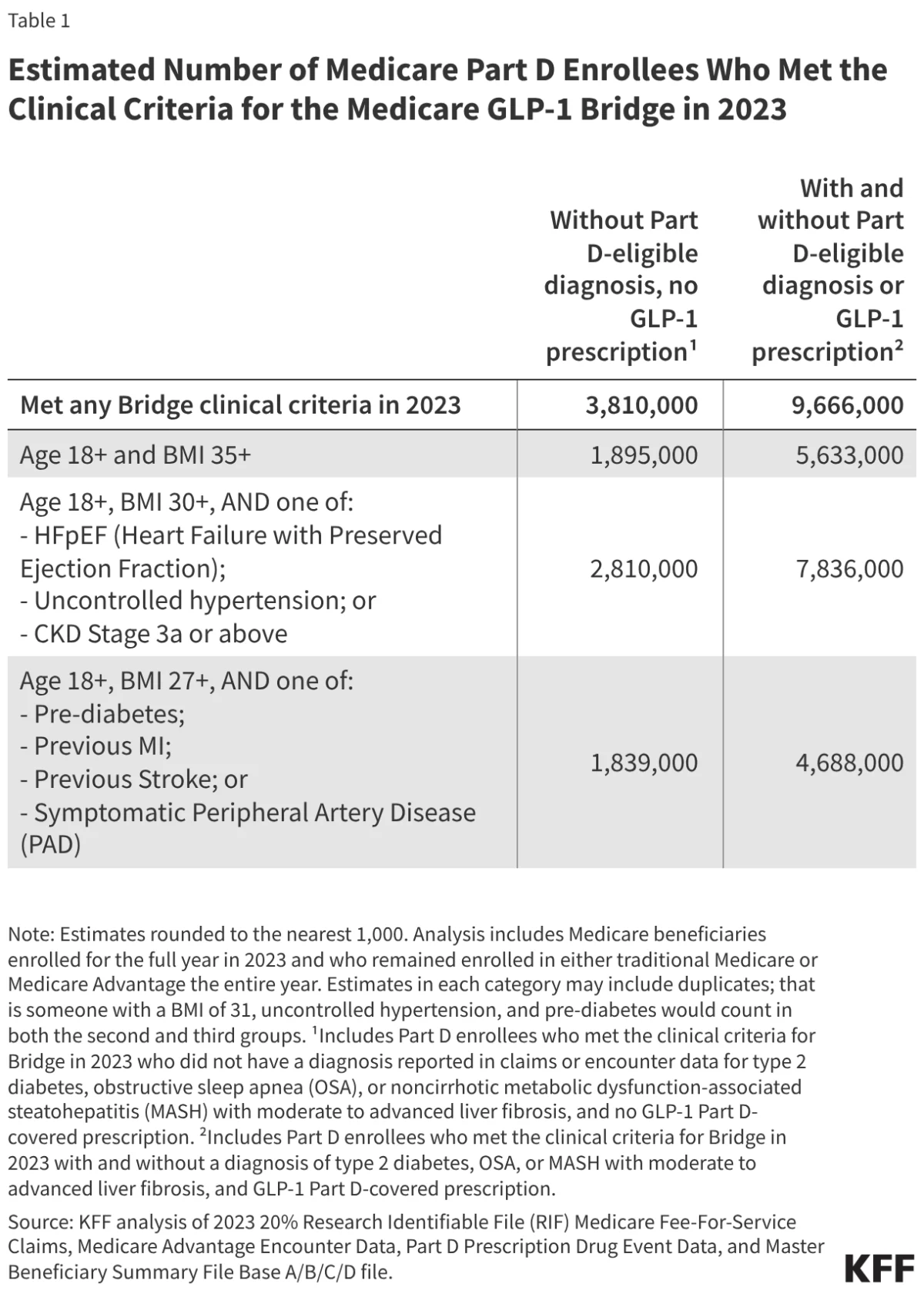
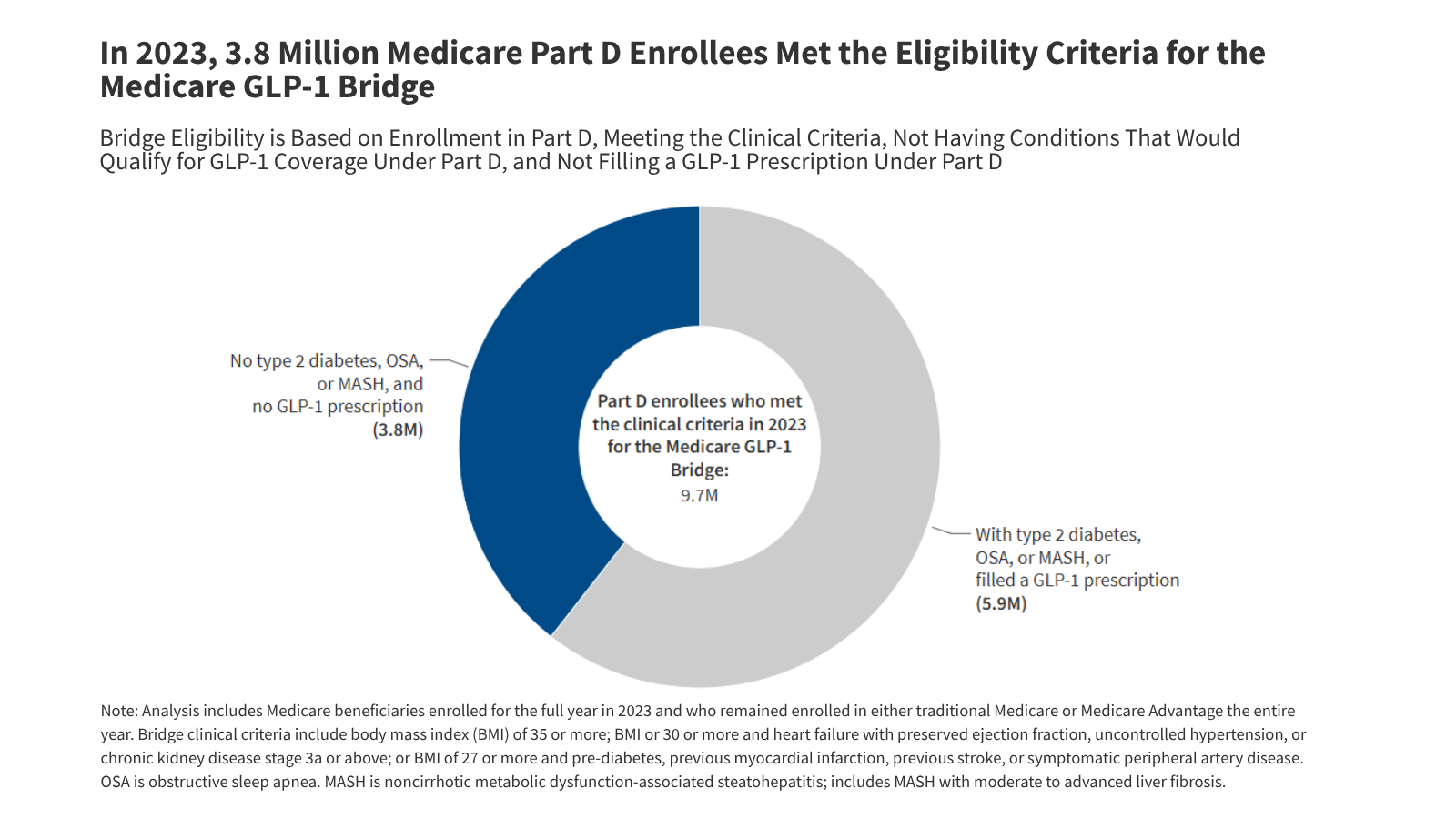
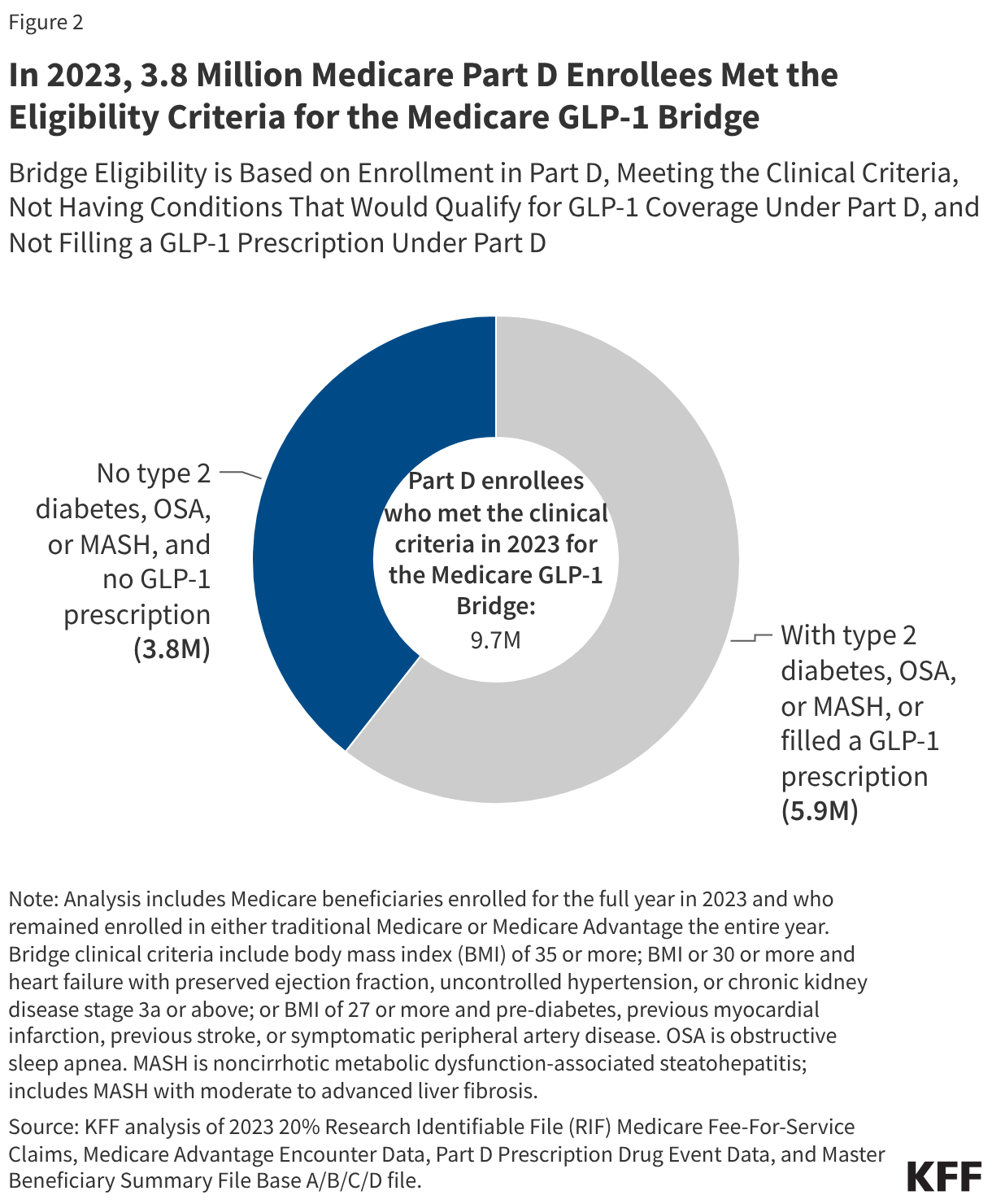
However, when filtering for the specific clinical criteria required by the Bridge, the number of "potentially eligible" individuals drops to approximately 3.8 million.
Why the Gap?
The discrepancy between the 13.3 million total and the 3.8 million eligible is largely due to the "exclusion" criteria. Of the 9.7 million Part D enrollees who met the clinical criteria, 5.9 million were disqualified because they already possessed a diagnosis of type 2 diabetes, OSA, or MASH—conditions that already qualify them for Part D coverage. This highlights the government’s focus on a very specific segment of the population: those who are severely affected by weight-related risks but currently have no other insurance-backed pathway to access these medications.
Official Responses and Perspectives
The response from CMS has been one of cautious optimism. Chris Klomp, the director of Medicare at CMS, has noted that the agency anticipates the program will serve "single-digit millions" of beneficiaries. This measured tone reflects the agency’s awareness of the immense financial risk involved.
Proponents of the program, including various medical associations, argue that the $50 copay is a necessary step toward addressing the "obesity-first" approach to preventive care. They argue that by managing weight effectively, the federal government may see long-term savings in the treatment of heart disease, stroke, and diabetes, which are currently among the most expensive conditions for Medicare to cover.
Conversely, some fiscal hawks in Washington have raised concerns about the long-term sustainability of such programs. They point to the "take-up" uncertainty. If 50% to 75% of the 3.8 million eligible beneficiaries participate, the cost to the federal government could reach as high as $10 billion over 18 months. These critics argue that without permanent savings, the program is a temporary fix that creates a budgetary cliff.
Implications for the Future of Medicare
The implications of the Medicare GLP-1 Bridge are profound. By testing this model, the government is essentially conducting a massive, real-world clinical and economic trial.
1. Clinical Shift
If the Bridge program demonstrates that beneficiaries who take these drugs experience fewer cardiovascular events or hospitalizations, it will provide the strongest evidence yet for a permanent legislative change. The "clinical criteria" approach may also set a precedent for how future high-cost, high-benefit medications are introduced into the Medicare system.
2. Market Impact
For pharmaceutical companies like Novo Nordisk (Wegovy) and Eli Lilly (Zepbound), the Bridge represents an opportunity to demonstrate the value of their products within the Medicare ecosystem. However, it also subjects them to intense scrutiny regarding pricing and long-term efficacy.
3. Financial Sustainability
The program’s success will be judged not just by weight loss outcomes, but by the "cost-offset" argument. If the $1.3 billion to $10 billion investment leads to a measurable reduction in other Part A and Part B spending, the political momentum for universal coverage of anti-obesity medications will become nearly unstoppable.
4. Administrative Precedent
The use of the Section 402 demonstration authority to bypass statutory prohibitions is a bold regulatory maneuver. If successful, it may encourage future administrations to use similar "bridge" programs for other emerging medical technologies that are currently excluded from Medicare, effectively modernizing the program through the back door of executive authority.
Conclusion
As July 2026 approaches, the Medicare GLP-1 Bridge stands as a testament to the evolving nature of healthcare policy in the United States. It is a bridge in every sense: a connector between current restrictive laws and a potential future of broader coverage, a bridge between scientific innovation and patient access, and a bridge between fiscal caution and the urgent need to address the health of an aging population.
For the 3.8 million Americans who fall into the eligibility criteria, the program offers a long-awaited tool in the fight against obesity. For policymakers, it offers a controlled environment to answer the most difficult question in modern healthcare: how to provide life-changing medical interventions without breaking the federal bank. Whether this initiative serves as a blueprint for the future or a cautionary tale remains to be seen, but one thing is certain—the impact of the Medicare GLP-1 Bridge will be felt for years to come.