For decades, the medical establishment viewed health outcomes primarily through the lenses of genetics, socioeconomic status, and individual lifestyle choices. However, a growing body of rigorous scientific research has shifted this paradigm, revealing that racial discrimination is not merely a social or political issue—it is a physiological one. Extensive peer-reviewed literature now confirms that systemic and interpersonal racism act as chronic stressors, fundamentally altering human biology, accelerating cellular aging, and driving profound health disparities across the United States.
The Biological Toll: Beyond "Sticks and Stones"
The impact of racism on health is often described through the concept of "allostatic load"—the cumulative wear and tear on the body resulting from chronic exposure to stress. When an individual experiences discrimination, the body’s stress-response system, primarily the hypothalamic-pituitary-adrenal (HPA) axis, is activated. While this system is designed to handle short-term threats, the repetitive, persistent nature of racial discrimination forces the body into a state of constant, high-alert inflammation.
Research published in journals such as Brain, Behavior, and Immunity and the Journal of Racial and Ethnic Health Disparities highlights how this physiological constant leads to systemic inflammation. Chronic inflammation is a known precursor to a host of cardiometabolic diseases, including hypertension, heart disease, and diabetes. As noted in the Cleveland Clinic guidelines, persistent inflammation can damage healthy tissues and organs over time, effectively "weathering" the body—a hypothesis first proposed to explain why Black women, in particular, face higher risks of adverse pregnancy outcomes and preterm births compared to their white counterparts.
A Chronology of Evidence: From Sociological Theory to Molecular Proof
The scientific understanding of this phenomenon has evolved significantly over the last 25 years.
- 2000: The Theoretical Framework: Camara Phyllis Jones introduced the "Gardener’s Tale," a seminal framework in the American Journal of Public Health that categorized racism into institutionalized, personally mediated, and internalized levels. This provided researchers with a vocabulary to measure how these layers impact health.
- 2005: Standardizing Measurement: The development of the "Experiences of Discrimination" scale by Nancy Krieger and colleagues provided the necessary validity and reliability for population-level research, allowing scientists to move beyond anecdotal reports to quantitative data.
- 2010s: The Biological Breakthroughs: Research began to move from self-reported health to biomarkers. Studies in Psychoneuroendocrinology and Health Psychology demonstrated direct correlations between discrimination and telomere shortening—the protective caps on chromosomes that indicate cellular age. The BeWELL Study (Black Women’s Experiences Living with Lupus) and the CARDIA Study (Coronary Artery Risk Development in Young Adults) provided hard data showing that women who faced high levels of discrimination exhibited faster rates of biological aging and increased disease activity.
- 2020s: Neural and Genomic Evidence: Recent studies have expanded into neuroscience and genomics. Research in JAMA Psychiatry and Biological Psychiatry has shown that Black women exposed to trauma exhibit altered neural responses to threat and changes in white matter microstructure. Simultaneously, 2025-era research published in The FASEB Journal has begun identifying genome-wide transcriptome differences linked to perceived discrimination, suggesting that the experience of racism may actually influence how genes are expressed within the human body.
Supporting Data: The Scope of the Crisis
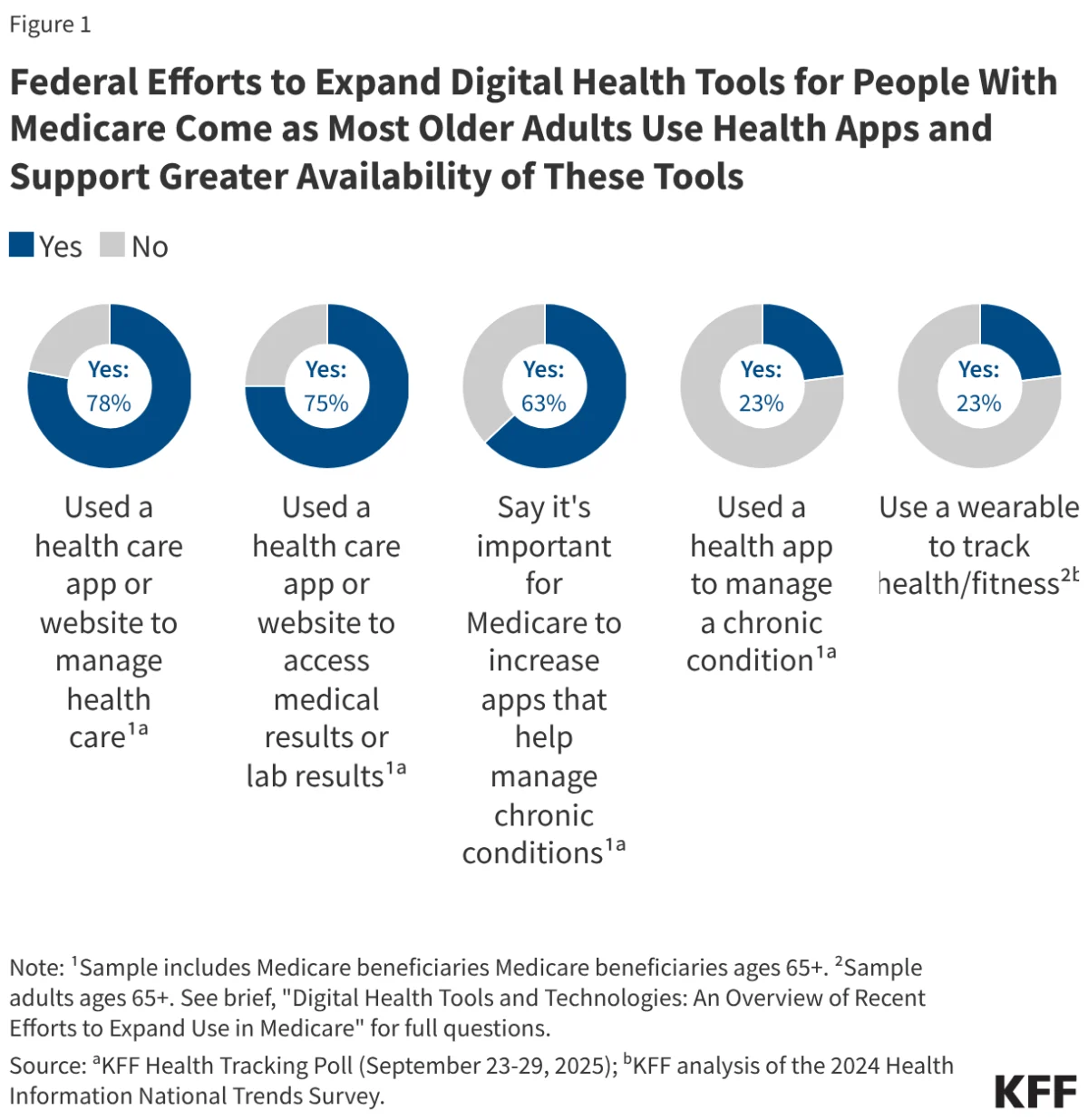
The data confirming these disparities is overwhelming. According to reports from the Kaiser Family Foundation (KFF), the economic burden of racial, ethnic, and educational health inequities in the U.S. is measured in the hundreds of billions of dollars annually.
The scope of the problem spans all demographics:
- Adolescence: Studies show that racial discrimination in youth predicts internalizing and externalizing symptoms, sleep disturbances, and even suicidal ideation. For many, the digital age has exacerbated this, with online racial discrimination emerging as a potent stressor for Black adolescents.
- Pregnancy and Birth: Systematic reviews confirm that exposure to racism is a primary determinant of adverse pregnancy outcomes. This is not restricted to socioeconomic status; even Black women with high educational attainment and financial stability face elevated risks, a phenomenon that underscores the pervasiveness of the "superwoman schema"—the societal expectation that Black women must be resilient and self-sacrificing, which paradoxically leads to higher allostatic loads.
- Aging: For older adults, the cumulative effect of a lifetime of discrimination manifests as an increased risk of all-cause mortality, cerebrovascular disease, and cognitive decline.
Official Responses and the Policy Landscape
The medical community has begun to officially recognize racism as a public health crisis. However, the policy response remains fraught with tension. While many health organizations have launched diversity, equity, and inclusion (DEI) initiatives to address these gaps, the political environment has grown increasingly hostile to such efforts.
Recent reports from KFF have tracked a significant trend: the elimination of federal diversity initiatives. This rollback threatens to undo years of progress in addressing health equity. Experts warn that dismantling these programs will not only reduce representation within the healthcare workforce but also hinder the ability of public health institutions to collect the very data necessary to identify and mitigate racial health disparities. The irony, as noted by researchers, is that while science has become increasingly precise in mapping the biological damage caused by racism, the institutional support required to address these root causes is currently under systemic attack.
The Implications: A Call for Structural Change
The implications of this research are profound. If racial discrimination is a root cause of illness, then the prescription for better health outcomes must extend far beyond the clinical setting.
1. Re-evaluating Clinical Practice
Physicians must be trained to recognize the "weathering" effects of racism. This involves integrating questions about discrimination into patient history taking and acknowledging that a patient’s high blood pressure or systemic inflammation may be a physiological response to social conditions rather than purely a genetic predisposition.
2. Addressing Structural Racism
The research suggests that individual "coping" mechanisms are insufficient. As shown in studies on "John Henryism"—a strategy of high-effort coping—the drive to overcome systemic barriers often comes at a high biological cost. True health equity requires structural changes in housing, education, and employment, as these are the environments where "everyday discrimination" is generated.
3. Protecting Data and Research
Given the current climate of legislative hostility toward diversity initiatives, there is an urgent need to protect public health research. Longitudinal studies, such as the CARDIA and BeWELL cohorts, are essential to proving the long-term impact of systemic policies. If we lose the ability to track these outcomes by race and ethnicity, we lose the ability to see the epidemic itself.
4. Moving Toward Holistic Health Policy
The "economic burden" argument serves as a bridge for policymakers. By framing health equity as a matter of national economic stability, advocates are attempting to shift the conversation. When a significant portion of the population is systematically stressed into chronic illness, the entire nation suffers from lost productivity, increased healthcare costs, and diminished social capital.
Conclusion: A Turning Point for Public Health
The evidence is no longer "hidden." From the shortening of telomeres in the DNA of young adults to the altered neural pathways in the brains of trauma-exposed individuals, the body keeps the score of racial discrimination. The challenge for the next decade is not discovering whether racism affects health—that question has been answered with resounding, scientific finality. The challenge is whether society has the political will to dismantle the systems that are literally making people sick.
As we move forward, the integration of these findings into public policy, clinical training, and social discourse is the only path toward closing the gap. We are witnessing a fundamental shift in our understanding of human biology, one that demands a departure from the myth of the "equal playing field" and an admission that, until we address the stressors imposed by systemic racism, the promise of equal health outcomes will remain out of reach.